
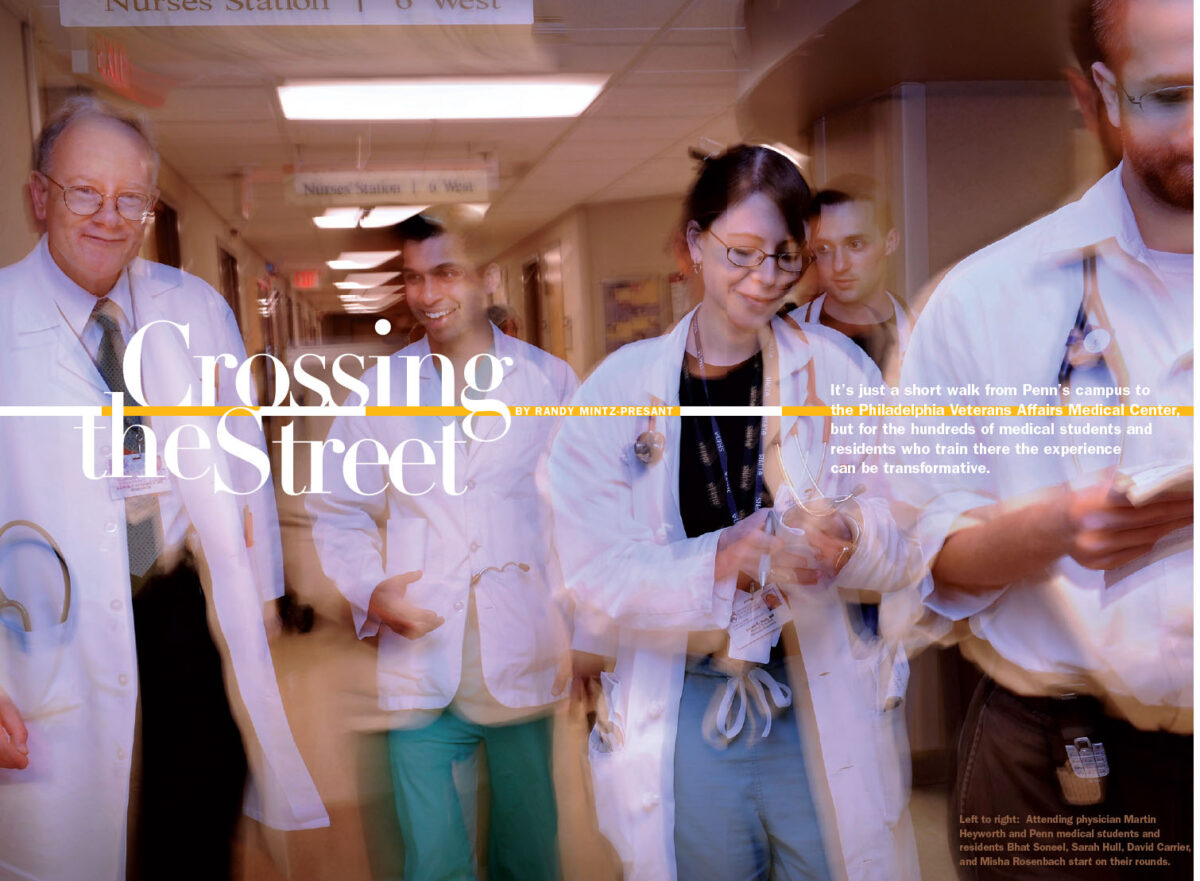
It’s just a short walk from Penn’s campus to the Philadelphia Veterans Affairs Medical Center, but for the hundreds of medical students and residents who train there the experience can be transformative.
By Randy Mintz-Presant | Photography by Candace diCarlo
Dr. Laura Mariani arrives early one Saturday at the Philadelphia Veterans Affairs Medical Center hauling two bags of groceries. As she unpacks them, she explains a PVAMC “tradition.” On weekends, the attending physician brings breakfast for the residents and students. Then, they all meet before going together on rounds. It’s a small gesture, but one that illustrates the appreciation PVAMC has for its Penn Medicine trainees.
The medical discussion that accompanies the juice and muffins is more telling. It shows the significant role the trainees have in patient care at PVAMC, the wide range of serious health issues they treat, and why their experience there can be so valuable.
Mariani leads the discussion, but everyone contributes. Second-year-student Deddeh Ballah reports that despite numerous tests, they can’t find an explanation for a 66-year-old patient’s nearly 70-pound weight loss. Dr. Vikram Prasanna, a resident, suggests testing the now 93-pound man for HIV. Mariani agrees, but also recommends looking at his living situation for signs of abuse and checking for heroin use. Then they move on. Another patient, whom Mariani remembers from previous years as a “really nice guy,” has a history of cocaine abuse and is in for severe abdominal pain. She agrees that they should test for lymphoma. A 52-year-old man is ready to be released, but as Prasanna notes, “he loves being here.” He is homeless, so she will work with PVAMC social workers to find him shelter. Daniel Caroff, a third-year medical student, shares his joy over an 86-year-old man who came in unresponsive but is now eating and talking. A more seasoned doctor, who knows the patient, wryly notes that they are in “the window between sedation and agitation.” The meeting continues for about 45 minutes, covering a multitude of physical, social, and emotional issues. Then Mariani asks in an upbeat voice, “Should we go see some patients?”
As they enter the hallway, the real costs of war and poverty are evident. Patients in wheelchairs maneuver through the corridors. Many are missing limbs. One wears a “Vietnam Veteran” baseball cap. Another has a small American flag mounted on his chair. One, who is walking, has the telltale eyes that come from years of living on the street. It’s a look that a hospital gown and shower can’t hide.
Patients, doctors, and nurses stop in the hallway to talk and joke with each other. Mariani leans over a wheelchair and rubs a patient’s shoulders. She helps another with his oxygen tubes. All the while, the residents are observing and helping. The atmosphere feels almost informal, more dorm-like than institutional. Yet when they enter the patients’ rooms, the mood turns serious. Mariani introduces herself as “Laura,” explaining that she is the attending doctor, and that the trainees are her “team.” Together they examine patients, asking questions and responding to concerns about such basic functions as eating and breathing.
One man’s legs are so swollen that he says, “I got a 20-pound foot,” and doesn’t seem to be exaggerating. Mariani and her team put on gloves and carefully unwrap the layers of gauze covering his legs. They examine the many sores and talk to him about his past care at other hospitals. When they are done, he asks them to cover his legs until they can be wrapped again, explaining that the sores, if left uncovered, will attract flies—perhaps recalling an experience from his past. Mariani, a pretty woman less than half his age, thanks him as they leave. “Anytime, I love you,” he calls back. Afterward, the doctors, clearly upset that the condition has gone this far, head to the computers to see what they can learn about the man’s medical history. After scrolling through many years of treatment, they decide to call the previous, non-VA facilities where he received care to discuss his condition.

William Heggs and Mrs. Frances Lloyd are among the thousands of veterans who receive care each year at PVAMC; Theresa V. Liggett (behind Mrs. Lloyd) works there.
Last year, more than 200 Penn medical students and 600 of its residents trained at PVAMC. For more than 25 years, Penn has provided PVAMC with resources and personnel, leading to a mutually beneficial relationship. It is one of 107 medical schools and 55 dental schools across the country affiliated with a VA facility. More than half of the physicians practicing in the United States had some of their professional education in the VA health care system. Yet many say that the size, depth, and extent of the Penn-Philadelphia VA affiliation are unique. Many Penn doctors maintain offices and see patients at PVAMC, or as they call it, “across the street.”
Ask the trainees what’s so important about the time they spend at the much smaller center, and most will tell you about the VA’s extensive data and its expertise in specific areas of research and clinical care. Listen longer and you’ll often hear about something less tangible but in many ways even more powerful.
Residents speak feelingly about African-American World War II veterans who risked their lives for a country where they were banned from lunch counters, Vietnam veterans ravaged from lives spent on the street, and Iraq veterans as young as they are who are scarred by stress disorders and trying to function without limbs. The stories abound. In today’s world of fast-paced, cost-driven medicine, what’s perhaps most remarkable is that these novice doctors have time to hear the stories. With all the talk about incorporating “humanism” in medical school curriculums, this is how the real education happens.
Dr. Karen Warburton, medicine residency director, says that she always tells new residents about a World War II veteran she met when she was training at PVAMC 10 years ago. While many of the patients, especially the older ones, treated female interns with skepticism and often outright chauvinism, this man was a “gentleman.” She earned his trust and quickly developed a good relationship with him. Yet it took more than a year for her to find out that this small, humble 85-year-old man had once been a fighter pilot decorated for his service. “He brought me this article one day,” she says. “He was a real hero. I had known him for more than a year, and he never even mentioned it. I always keep that article in my office and show it to residents.”
Humility and service are values you hear about a lot at the VA. Residents talk about how appreciative the veterans and their families are, something Dr. Neil Fernandes, a first year resident, attributes to the “kind of personality and selflessness it takes to serve your country.”
The students and residents who do best at the VA seem to share some of that selflessness, or at least are not, as one physician says, “prima donnas.” There are few frills here. Getting a full-size refrigerator and microwave to improve on-call meal options for residents was significant enough to warrant mention in the 2008 Annual Report. Prior to that, Warburton says, residents working overnight had to head to a dungeon-like storage area for often less-than-appetizing options. “You learn to laugh,” she adds. While part of that comes from being the kind of person who makes the best of things, it is something the medical trainees also learn from the veterans. It is hard to complain about a bad dinner when someone your own age, who could be facing a lifetime of crippling back problems from wearing 50 pounds of body armor in the Iraqi heat, isn’t complaining.
“They all have colorful and perhaps more meaningful stories and experiences than most of us will ever have,” says Warburton. “We often see them at their worst and see what disease has done,” she adds quietly.
PVAMC trainees not only work closely with their attending physicians on diagnosis and treatment decisions but also gain experience from counseling patients and families. Because the facility is smaller and has fewer support personnel than a large academic medical center such as the Hospital of the University of Pennsylvania, they say, the pace is a little slower, which allows more time for such conversations.
“[Trainees] can spend two hours talking to a patient about diabetes—what it means, how to take care of yourself,” says Warburton. “Patients often have a number of physical and social issues. It’s like a crash course in internal medicine.” Residents see firsthand how social-economic factors such as education and income affect physical health.
“One of the things we recognize is poverty as a cause of illness,” says Dr. David Asch GM’87 WG’89, executive director of the Leonard Davis Institute of Health Care Management and Economics and the Eilers Professor of Health Care Management and Economics. Patients often present with chronic diseases in much more advanced stages than at other facilities. “We often catch people who have fallen through the cracks,” says Asch. “The VA does a good job of taking care of the veterans who walk through its doors, but by the time they get here it may be late.”

Asch trained at PVAMC as a resident and has been involved with it throughout his more than 20 years on Penn’s faculty. In 2001, he founded CHERP, the Center for Health Equity Research and Promotion. Areas of research include chronic illnesses such as diabetes and hypertension, mental illness, joint replacement, and pain management. A partnership with the University of Pittsburgh, CHERP is now the Department of Veterans Affairs’ national program on health disparities. It has grown to become a highly respected, multi-faceted organization with a nearly $10 million annual budget; its 34 core investigators focus on understanding and eliminating disparities caused by social and cultural forces. “Health care is not the only thing required for health,” Asch says, pointing out the important roles social support and education play.
By providing essential services to the Philadelphia region’s large veteran population, PVAMC helps alleviate some of the pressure on the city’s health system, Asch says, noting that it’s “the closest thing Philadelphia has to a public hospital.” When patients need services not provided at the VA, such as maternity or radiology, they will be treated at a Penn Medicine facility. In addition to having 140 acute-care beds and a 220-bed nursing home, PVAMC provides extensive outpatient care as well as housing information, education support, and other services; part of what Asch calls its “social mission.” Last year, nearly 68,000 veterans were treated on an outpatient basis at PVAMC or one of its four community-based clinics. The center received $9 million in federal stimulus funds through the American Recovery and Reinvestment Act of 2009, which it will use primarily to upgrade and increase the capacity of its emergency room.
PVAMC has developed an expertise in treating and providing services to patients who are homeless or have spent time living on the street. In April, the VA Central Office announced that it was establishing a National Center on Homelessness among Veterans at PVAMC. It will be a joint initiative with a VA medical center in Tampa, Florida; Penn and the University of South Florida will provide support. While the VA has provided extensive outreach and case management for homeless veterans across the country since 1987, this will be its first initiative to conduct research and develop policy on the issue.
The Philadelphia region has one of the highest concentrations of veterans in the country, with close to 330,000 in the city and six surrounding counties. Of those, more than 94,000 are enrolled at PVAMC, a nearly 30 percent penetration rate that is especially impressive because not all veterans are eligible for coverage. (Enrollment criteria include financial and medical need, military record, and whether or not a disability is service-related.) A number of government and civic leaders have proposed expanding eligibility to help address our nation’s current health care and economic issues. They say this is particularly important now, given the high percentage of military personnel from low-income backgrounds, compared with the draft era.
In 2004, Congress granted all Iraq and Afghanistan war veterans five years of free health care following active duty. The Philadelphia VA now has almost 2,200 vets from those conflicts enrolled, a 47 percent increase from 2006. It expects the numbers to increase even more this year, with the planned return of many Pennsylvania and New Jersey National Guard units.
To serve these returning veterans, PVAMC expanded its Operation Enduring Freedom and Operation Iraqi Freedom (OEF/OIF) program so that it could provide more comprehensive case-management and social-work assessments. It has also received funding to increase the staff and equipment of its interdisciplinary polytrauma team, which addresses the severe, multiple injuries that many OEF/OIF veterans sustained from explosions and blasts. These include traumatic brain injury, amputation, visual impairment, and post-traumatic stress disorder.
The influx of OEF/OIF veterans means that PVAMC is now treating more women and younger veterans than ever before. Its Women’s Health Clinic offers mammograms, Pap tests, infertility referrals, and other services. Across the country, the VA system began providing medical and psychosocial services for women in 1988, when women represented just 4.4 percent of all veterans. Last year, women made up 11 percent of OEF/OIF veterans nationally, and it is estimated that by 2010, more than 14 percent of all veterans will be women. Nearly 67 percent of the women who use VA health services across the country are under 30, compared to less than 59 percent of men.
One of the goals of offering Iraq and Afghanistan veterans free health care is to help them avoid some of the health problems now faced by aging Vietnam vets by starting them on a lifetime of preventive care. The VA is considered one of the most accomplished primary-care providers in the country. Its electronic health-records system is often cited as a model for facilitating comprehensive continuity of care across locations and over time. Physicians know when to remind patients about screening tests and can easily access data from previous tests, an advantage not lost on trainees. “It’s more navigable and almost seamless,” says Dr. Judd Flesch C’01 M’06, a third-year resident, describing the benefits of using one system to order, conduct, report, and evaluate medical tests. As residents make their rounds, they frequently stop at a computer to check a patient’s medical history.
The electronic health-records system dates back more than 20 years, arising from the need to serve a large, mobile patient population, and it gives Penn researchers access to essential longitudinal data that they say they could not get elsewhere.
“You can’t do outcomes research without a strong retrospective data base,” says Dr. Glen Gaulton, executive vice dean and chief scientific officer for the School of Medicine, who notes that the relationship with PVAMC benefits Penn research in numerous ways. It provides Penn with “access to a distinctive patient population” that supports its work in areas such as mental health and geriatrics. Penn physicians are directly involved in the Philadelphia VA’s special programs on Parkinson’s disease, mental illness, and other conditions. This has given Penn a “head start” in preparing to treat our nation’s aging population, says Gaulton, and it is now “ahead of the curve because we had to address it.”
Working so closely with a large public-health system has also helped to make Penn a leader in health-service research. Gaulton cites as an example the work of Dr. Margaret G. Stineman GM’87, vice chair and director of research in the Department of Rehabilitation and Physical Medicine, and her colleagues on patient classification, which is the basis for current Medicare procedures and has been used to establish industry measures on inpatient rehabilitation, patient mobility, and quality of life.
“The VA is probably the only large mental-health system in the country,” says Dr. David W. Oslin GM’01, associate professor of psychiatry at PVAMC and Penn. Unlike physical medicine, most mental health clinics are still “very isolated,” he says. “They function essentially as individual practices. There’s little integration.” At the VA, there is “a lot more integration and dialogue between physicians working in primary care and psychiatry. It’s the same records, same system.”
Penn’s affiliation with PVAMC provides data that is key to Oslin’s substance-abuse work, which includes research on connections between alcohol dependence and mental illnesses such as depression, he says. “We do 60,000 alcohol screens a year at this facility and there are 3.5 million screens through the nation’s whole [VA] system.” Many veterans participate in Penn clinical trials on such issues as suicide prevention and post-traumatic stress disorder, helping both patients and researchers.
Another benefit of the affiliation is that young doctors are “being exposed to different cultures and ways of doing medicine,” says Oslin. “Their career development isn’t monolithic. This is a fully integrated public-health system. They can take bits and pieces of it and move the field along.” He adds that this is particularly timely now, with health reform prominent on the national agenda and more and more medical schools trying to build system-development into their curriculums.
Dr. Rachel Bennett, a first year intern in psychology, says that PVAMC’s “holistic view” is something she will take with her when she practices. “There is a social mission to help with [veterans’] lives,” she says, explaining how that means working with social workers, veterans’ families, primary-care physicians, and any needed specialists. She says she has treated young Iraq veterans with “post-traumatic stress disorders so bad they have to be hospitalized and can’t hold jobs or relationships,” and notes that it is not unusual for her to spend more than an hour talking to one of them about their experiences and issues. She talks solemnly about how these veterans, the same age as she is, have already sacrificed so much. Eventually, Bennett wants to work with children and adolescents who are victims of severe trauma and abuse. She says that her PVAMC training has helped prepare her, noting that the nightmares and inability to trust are shared by both groups.
Bennett and most other residents say that learning how to counsel patients, being empowered to make decisions, and gaining hands-on experience provide invaluable training. With no overnight phlebotomy service, residents become accustomed to drawing blood. They develop strong relationships with patients and are often the ones asked to deliver bad news or console a family. When staff is short, they might even have to transport patients for tests. “Most hospitals are much more ‘top-down,’” says Flesch. “I’m approaching the end of my medical training and this will make me a better attending physician.” He says that spending time with patients has improved his clinical judgment, for example by making him more aware of the importance of not just relying on an echocardiogram but “paying attention to the physical exam and what’s going on in the heart.” When Mariani leads residents on rounds, she points out how she uses all of her senses to evaluate patients—listening to their breathing, noting how a sore smells, feeling the skin, etc.
Doctors say that being “hands on” and having more autonomy leads to innovation and improvements in care. Dr. Samuel Kuna M’06, associate professor of medicine and chief of the pulmonary, critical care, and sleep section at PVAMC, says that at the VA he has been able to experiment with many new programs, such as group sessions for clinical management. While that program ultimately saved money, Kuna says it would have been difficult to try it in a system dependent upon third-party payers and using established billing codes and procedures. PVAMC opened an on-site sleep center in 2003 to serve the increasing number of veterans suffering from stress-related sleep disorders. It treated more than 1,800 veterans in 2008 with inpatient and home-based programs that monitored their sleep and used combinations of talk, drug, and behavioral therapies.
As a training site for future medical leaders, Penn is known for providing access to state-of-the-art technology, cutting-edge research and world-renowned physicians. Students and residents who do a rotation at PVAMC say they also benefit from something simpler but often transformational: time to spend with a special group of patients, from whom they learn firsthand what it takes to be a doctor. It is, says Judd Flesch, “a special privilege to help veterans.”
Randy Mintz-Presant is a freelance writer in Philadelphia.



